When and where to start planning pregnancy?
Pregnancy is a very important moment in the life of a woman, and of the family as a whole. It brings not only joyful...
Thank you
The site provides reference information for informational purposes only. Diagnosis and treatment of diseases should be carried out under the supervision of a specialist. All drugs have contraindications. Expert advice is required!
 Under normal conditions for KTG ( cardiotocography)
a number of parameters are recorded that must be taken into account when evaluating the results of the study.
Under normal conditions for KTG ( cardiotocography)
a number of parameters are recorded that must be taken into account when evaluating the results of the study. When CTG is evaluated:
In the study of CTG, there are:
Instantaneous oscillations can be:
Slow oscillations
As for slow oscillations, they are characterized as changes in the fetal heart rate within one minute. On CTG, they appear as small waves with sharp teeth.
Depending on the nature of slow oscillations, CTG can be:
Also, when assessing slow oscillations, their number is taken into account, that is, how many times the heart rate increased or decreased ( ) in a minute.
On KTG can be registered:
Fetal movements are determined on the lower line of the cardiotocogram, which registers uterine contractions. The fact is that uterine contraction is recorded by a sensor that measures the circumference of a woman's abdomen. When the uterus contracts, the circumference of her abdomen changes somewhat, which is determined by a special sensor. At the same time, when moving ( movement) of the fetus in the uterus, the circumference of the abdomen may also change, which will also be recorded by the sensor.
Unlike uterine contractions ( which on the lower line of the cardiotocogram look like smoothly increasing and also smoothly decreasing waves), fetal movements are determined in the form of sharp rises or jumps. This is due to the fact that when the uterus contracts, its muscle fibers begin to contract relatively slowly, while the movements of the fetus are characterized by relative speed and sharpness.
The reason for the absence or mild fetal movements may be:
Measurement of the tone and contractile activity of the uterus is called tocography. Tokography can be external ( is part of the CTG and is carried out using a strain gauge installed on the surface of the mother's abdomen) and internal ( To do this, a special sensor must be inserted into the uterine cavity.). It is possible to accurately measure the tone of the uterus only with the help of internal tocography. However, perform it during pregnancy or childbirth ( i.e. before the baby is born) impossible. That is why, when analyzing CTG, the tone of the uterus is automatically set to 8 - 10 millimeters of mercury. In the future, when registering the contractile activity of the uterus, indicators that exceed this level are evaluated.
During the training bout, there is also a slight contraction of the uterus and an increase in its size in the bottom area, which is captured by a sensitive strain gauge. At the same time, the same changes will be noted on CTG as in normal contractions, but less pronounced ( that is, the height and duration of the curvature of the bottom line will be smaller). In terms of duration, the training bout takes no more than a minute, which can also be determined on the graph.
Sinusoidal rhythm is characterized by:
Normally, STV should be more than 3 milliseconds ( ms). With a decrease in this indicator to 2.6 ms, the risk of intrauterine damage and fetal death increases to 4%, and with a decrease in STV less than 2.6 ms, up to 25%.
Many different scales have been proposed, but the most common today is the Fisher scale, which is considered the most reliable and accurate.
The assessment of CTG on the Fisher scale includes:
Fisher's scale in the Krebs modification when assessing CTG
Estimated parameter | Number of points |
||
1 point | 2 points | 3 points |
|
Basal Rhythm | Less than 100 beats per minute. | 100 - 120 beats per minute. | 121 - 159 beats per minute. |
Over 100 beats per minute. | 160 - 180 beats per minute. |
||
Amplitude of slow oscillations | Less than 3 beats per minute. | 3 to 5 beats per minute. | 6 to 25 beats per minute. |
Number of slow oscillations | |||
Number of accelerations | There are no accelerations. | 1 to 4 sporadic ( random) accelerations in 30 minutes. | More than 5 sporadic accelerations in 30 minutes. |
Decelerations | late or variable. | late or variable. | Missing or early. |
Number of fetal movements | None. | 1 - 2 movements in 30 minutes. | More than 3 movements in 30 minutes. |
Evaluation of CTG according to the FIGO method
Criterion | Interpretation of results |
||
Norm | Prepathology ( "suspicious" CTG) | Pathology |
|
Basal Rhythm | 110 - 150 beats per minute. | 100 - 109 beats per minute. | Less than 100 or more than 170 beats per minute. |
151 - 170 beats per minute. |
|||
Rhythm variability | 5 - 25 beats per minute. | 5 - 10 beats per minute for 40 minutes. | Less than 5 beats per minute. |
sinusoidal rhythm. |
|||
Number of accelerations | More than 2 within 40 minutes. | Missing for 40 minutes. | Absent at all. |
Decelerations | Absent or single variable. | Variable. | Variable or late. |
The Dawes-Redman criteria include:
If the monitor displays the inscription “criteria not met”, then one or more of the listed indicators does not correspond to the norm. In this case, the study should continue for at least 40 minutes. If the inscription "criteria met" does not appear, there may be a violation of the condition of the fetus in the womb. At the same time, a more detailed examination of the woman is recommended, as well as the repetition of CTG in dynamics ( same day or next day).
PSP calculation during pregnancy can determine:
A non-stress test can be:
 There are a number of pathological conditions that can be identified using the correct decoding of CTG. The sooner pathological changes are detected, the sooner the doctor will take measures to eliminate them, which can save the life of the child.
There are a number of pathological conditions that can be identified using the correct decoding of CTG. The sooner pathological changes are detected, the sooner the doctor will take measures to eliminate them, which can save the life of the child. The cause of fetal bradycardia can be:
With acute ( rapidly developing) hypoxia, it is extremely important to diagnose and eliminate it in time, since otherwise damage to the fetal nervous system and death of nerve cells of the central nervous system may occur ( central nervous system), which can cause developmental disorders or even intrauterine death of the fetus. That is why any doctor conducting CTG should be able to recognize the main signs of hypoxia.
The presence of fetal hypoxia may indicate:
On CTG, this can be manifested by alternating sharp rises in heart rate ( characteristic of the initial stage of hypoxia), which are immediately followed by sharp decreases in heart rate ( characteristic of more severe hypoxia). These changes are associated with fetal movements recorded on the tokogram. The detection of such changes is an indication for urgent delivery by caesarean section, since otherwise irreversible damage to the nervous system of the fetus and its death are possible.
Although CTG cannot be used to diagnose oligohydramnios, the study may reveal signs of initial or severe fetal damage ( in particular, an increase or decrease in heart rate, signs of hypoxia, and so on), which may serve as a reason for a more detailed examination of the woman. If, against the background of a “bad” CTG, oligohydramnios is detected, the issue of premature delivery should be raised. At the same time, it is worth noting that even with confirmed oligohydramnios, a woman can have an absolutely normal cardiotocogram.
To make an appointment with a doctor or diagnostics, you just need to call a single phone number
+7 495 488-20-52 in Moscow
+7 812 416-38-96 in St. Petersburg
The operator will listen to you and redirect the call to the right clinic, or take an order for an appointment with the specialist you need.
Clinic name |
Monitoring the condition of the fetus is an important goal of examining a pregnant woman. It can be carried out in different ways. Cardiotocography is the most common, painless and affordable method of instrumental condition monitoring.
Cardiotocography is a technique for assessing the state of the fetus developing in the womb, which consists in analyzing changes in the frequency of its heartbeats at rest, during movements, and also in response to external factors.
Devices for conducting this study - cardiotocographs - are available in all antenatal clinics and maternity hospitals.
The methodology of this study is based on the well-known Doppler effect. The hardware sensor creates special ultrasonic waves that go inside the body and are reflected from the surface of media with different sound conductivity, after which they are fixed again by it. When the interface between media is shifted, for example, when moving, the frequency of the generated and received ultrasonic waves becomes different. The time interval between each heartbeat is the heart rate (HR).
The purpose of the CTG is the timely detection of abnormalities in the functional state of the fetus, which allows the doctor, if any, to select the necessary therapy, as well as choose the appropriate timing and method of delivery.
No special preparation is needed for this study.. But to obtain reliable results during the study, the woman must be relaxed and in a comfortable position, not to move. Therefore, before the procedure, you should go to the toilet in advance.
It is recommended that you eat approximately 2 hours before the test and should not be done on an empty stomach. By agreement with the doctor during the procedure, small snacks with something sweet are allowed if the baby is in the sleep phase in order to activate it. To do this, you can pre-purchase sweet food.
You should not take painkillers and sedatives 10-12 hours before the examination.
During the study, the expectant mother takes a position on the couch lying on the right or left side of the body or half-sitting, leaning on a pillow. Special meters are fixed on her stomach - a gel is applied to one and fixed in the place where the fetal heart beat is best felt, the other sensor, which registers excitations and contractions, is placed in the area of the projection of the right angle or the bottom of the uterus. The patient independently marks the periods of fetal movement using a button for registering fetal movements.
Monitoring is carried out for at least half an hour to get the most accurate information about well-being. This duration of the study is explained by the frequent alternation of the phases of sleep and wakefulness in the child.
Unlike many other research methods, the decoding of CTG at 32, 33, 34, 36, 37, 38, 39 and 40 weeks does not have any significant age-related nuances. There is a slight tendency to decrease the average fetal heart rate from 32, 33, 34 to 38 weeks.
One of the components of CTG recording is currently actography - recording fetal movements in the form of a graph. There are two ways to evaluate a child's movements. Mom can independently count the movements of the fetus that she feels. Or many modern devices are able to record movements themselves using a sensor. The second registration method is considered more reliable. At the same time, the movements look like high peaks on the actography graph.
The fetus moves almost constantly, except for periods of its sleep. According to CTG data, during 32.34, as well as 35-40 weeks of a normally developing pregnancy, the fetal motor activity generally increases. At 34 weeks, an average of 50 - 70 movements per hour are noted. After 34 weeks, an increase in the number of movements is recorded. So, from 60 to 80 movements per hour are recorded. The average duration of episodes of perturbations is 3-4 seconds. Gradually, with the growth of the fetus, it becomes more crowded in the uterine cavity, so closer to it it becomes calmer.
In addition to the fetal heart rate and its movements, CTG can register contractile movements of the uterus, that is, contractions. Recording contractions on CTG is called a tokogram and is also displayed as a graph. Normally, the uterus reacts to the movements of the fetus in it with its contractions (contractions). At the same time, a decrease in the child's heart rate is recorded on CTG in response to uterine spasms. Contractions are the main sign of upcoming labor. Based on the tokogram, the doctor can determine the strength of the contraction of the muscular layer of the uterus and distinguish false contractions from true ones.
Based on the foregoing, it can be seen that CTG is a very important examination of the state of the developing fetus in the womb, which allows you to obtain information about the state of the heart rhythm, movements, and even evaluate contractions. Any deviations in CTG require a thorough cumulative analysis by a competent specialist in order to take the necessary measures that can save the life of a little man. All these properties make CTG an indispensable type of examination.
A woman meets many studies for the first time, some diagnostic procedures are not familiar to her, therefore, the expectant mother is alarmed, they make her doubt that everything is in order with her and the baby. One gynecologist said that for the first time a young woman came to the CTG procedure all in tears, with the full conviction that once an examination was scheduled, then a pathology was suspected ... a specific purpose. So what is this procedure - ktg? Why is she appointed? Let's look into these issues in detail.
Cardiotocography (CTG) is a research method that is based on the analysis of the variability of the fetal heart rate (in medical terminology, the fetus is the unborn baby from the eighth week of intrauterine development until the moment of birth). With fetal CTG, the frequency of the baby's movements and the contractile activity of the uterus are also recorded. CTG is carried out using Doppler-based cardiac monitors, which record changes in the intervals between individual cycles of the fetal cardiac activity.
Analyzing the results of CTG, one can assess the functional state, frequency of fetal movements, understand whether he is comfortable, whether there is enough oxygen, the frequency and strength of uterine contractions. Thanks to the fetal CTG procedure, the doctor can timely notice deviations in the course of pregnancy and provide the necessary assistance to the pregnant woman and the unborn baby in time. Fetal CTG is prescribed both for prophylactic purposes from 30-32 weeks of pregnancy to all women, and for medical reasons (in this case, the terms may be different).
Usually, if the pregnancy is going well, a woman undergoes a CT scan of the fetus in the 3rd trimester at least twice, if there are indications (aggravated obstetric history, entanglement of the umbilical cord, scars on the uterus, placental insufficiency, polyhydramnios or oligohydramnios, features of the development of the fetal cardiovascular system) - more often according to doctor's instructions. With planned hospitalization a few weeks before childbirth, women undergo daily fetal CTG, this procedure becomes familiar to them, and most are looking forward to it, because it shows the heartbeat of their crumbs, some devices reproduce the sound of the baby's beating heart.

Fetal CTG is completely painless for both the expectant mother and her future baby. A woman occupies a comfortable position half-sitting or reclining on her back or on her side; lying down is not recommended for the procedure, because. in the supine position, compression of the inferior vena cava may occur and the recording results will be distorted. Two sensors connected to the monitor are attached to the belly of the pregnant woman. One sensor captures the fetal heartbeat, and the second - uterine contractions.
Older heart monitors have another fetal movement sensor with a button that is placed in the woman's hands and she has to press the button every time she feels her baby move. New modern devices do not have such a device. The procedure lasts 30-35 minutes, so before it is carried out, the woman is recommended to get enough sleep, go to the toilet. If the child during the CTG is not active and sleeps in the mother's stomach, the procedure will not be informative.
To increase the activity of the fetus, a woman in the absence of allergies is recommended to eat one or two slices of chocolate. It is not recommended for a woman to worry, get upset, worry, these factors can contribute to the distortion of the results. The fetal CTG procedure is completely harmless, painless, has no contraindications and side effects from both the mother and the fetus. Also, fetal CTG can be carried out directly in childbirth in order to understand how the baby feels.

Deciphering the CTG of the fetus is the prerogative of gynecologists, but every woman can have an idea of \u200b\u200bwhat the results of the CTG mean, what the indicators are and whether they are the norm of the CTG. As a rule, by the 32nd week, the child’s cardiac reflex has already been formed, and for every movement he has a reaction of the cardiovascular system in the form of an increase in heart rate. Sensors record these indicators, which are recorded as a curve on a tape - a cardiotocogram. The gynecologist evaluates the curve in points from 1 to 10. According to this assessment, it can be concluded how the child feels in utero, how much his body, including the cardiovascular system, is provided with oxygen, whether there is fetal hypoxia.

It is difficult for an unprepared person to say what a cardiotocogram means. It shows a continuous line and teeth, directed mainly upwards, less often downwards. But how to decipher these indicators? On the cardiotocogram of the fetus, the doctor evaluates the following indicators:

For each of the four indicators, the doctor assigns points, from 0 to 2. And then, summing up the result, he receives the final number of points, which gives an assessment of the condition of the fetus and its cardiac activity.
Fisher's rating scale is as follows:
Normal CTG indicators are a concept that fits into very specific criteria, namely: the basal rhythm should be 119-160 beats per minute, the deviation amplitude is 7-25 beats per minute, at least 2 accelerations in 10 minutes, the absence decelerations or mild decreases in heart rate. These are normal indicators. But you should always remember that one record does not make a diagnosis, and small deviations from the norm are not a pathology. The graph data may vary depending on whether the baby is sleeping or awake, is in a calm or active state, and also on which week of pregnancy the examination is performed.

The doctor should be alerted to the results of CTG, which have significant deviations from the normal range: if the basal rhythm is less than 110 or more than 190 beats per minute. A low frequency of 110 or less indicates a slowing of the heartbeat in the fetus, and a high one, on the contrary, indicates a pronounced increase. Both can indicate fetal hypoxia, oxygen starvation. A basal rhythm over 190 and under 110 is scored as 0 points. It is also not very good when there are no accelerations in response to the movement of the fetus. This may indicate tension and exhaustion of the fetal compensatory reactions, immaturity of the cardiac reflex.
Deep and frequent decelerations always alert the doctor, they may indicate a violation of placental blood flow and require careful study. A monotonically variable basal rhythm or an amplitude of less than 10 or more than 25 beats also raises questions for the doctor. If the decoding of fetal CTG gives a dubious result of 6-7 points, it is necessary to repeat the study and supplement it with other examination methods to determine the reasons that led to this result. But do not immediately panic, it can only harm the condition of the unborn baby.
The reason for the immediate hospitalization of a pregnant woman is threatening indicators on the Fisher scale 1 point - 5 points.

You are pregnant, you feel how your baby is growing, kicking, and your meeting with him will take place very soon, but the doctor has not yet prescribed CTG for you? Why? Perhaps your pregnancy is going well, and its term has not come to 32 weeks, you have no indications for an earlier pregnancy. This is just a reason for joy, and in no way a reason for concern.
No. If any deviations as a result of the procedure were identified, the doctor will refer you to other examinations (laboratory, instrumental). And already in a comprehensive assessment, taking into account the data of all studies, a diagnosis will be made, the results of deciphering the CTG of the fetus will be confirmed or refuted.
During the delivery period, strong muscle contractions of the uterus occur, which provoke the advancement of the fetus to the birth canal. At this point, the child's body is under severe stress. To monitor his condition during childbirth, a CTG device is connected to the mother's abdomen. Most women do not know that CTG contractions look different and can be a source of information about all the pathological changes during childbirth.
The first signs of the onset of labor are contractions
In this article you will learn:
The diagnostic method of CTG is an ultrasound procedure using a cardiotocograph. The essence of CTG is to graphically display the rhythm of contraction of the fetal heart muscles and the muscular tissue of the uterus. The data obtained during cardiotocography allow us to assess the risks of preterm birth or the likelihood of a danger to the life of the child during delivery.
CTG performed during childbirth shows:
During pregnancy, starting from the 32nd week, a woman is prescribed a periodic examination with a cardiotocograph. CTG without contractions is recommended for pregnant women for the timely detection of pathological conditions regarding the health of the fetus. The procedure allows you to determine the lack of oxygen supply, problems in the work of the heart, cord entanglement and neurological abnormalities in the fetus.

CTG shows the frequency of contractions
CTG during contractions, as a rule, is carried out after the first symptoms of the onset of labor. If a woman enters the admission department of the maternity hospital already with disclosure, then, of course, no preparation for the procedure is carried out, since it is not always possible to predict the onset of childbirth.
In the event that the woman was in the hospital, a caesarean section is expected, or the birth was caused by medications, preliminary preparation for cardiotocography is desirable.
Features of preparation for CTG:

It is important that during CTG the child is active
If in the process of conducting the study, inaccurate data are obtained or the result is unsatisfactory, the specialist may advise you to eat something sweet, change position, or drip a small amount of magnesia. All these methods will be aimed at increasing the physical activity of the fetus to determine accurate data.
A cardiotocograph is a device with sensors that are attached to the belly of a pregnant woman with straps and fixed at the location of the fetus. Ultrasonic waves are transmitted through the sensors, which travel the way to the fetal heart and back. The device to which the data is received correlates the frequency of uterine contractions with the heart rate of the child and produces a graphic image.
On the ribbon with graphic lines: tachogram and histogram. The first indicator is the frequency of the heart muscles of the crumbs, and the second is a display of the strength and frequency of contractions.
The procedure itself goes as follows:

The procedure is not complicated, it takes about half an hour.
During the procedure, which lasts 20-30 minutes, it is not recommended to change position, as the sensors on the abdomen may move and the study will have to be carried out again.
Cardiotocography during pregnancy and during childbirth is different. If a woman has begun labor activity, then contractions on CTG will clearly display the rhythm of contraction of the muscle tissue of the reproductive organ.
During contractions, CTG indicators change: fetal motor activity, basal and variable rhythm, acceleration, deceleration, uterine contractions.
A pregnant woman may have false (training) contractions or natural ones. Based on the results of the diagnostic data, the specialist can determine whether the birth actually occurs, or the body is just preparing for the birth of the baby.

Women often experience false contractions.
The main difference between false contractions and real contractions is the absence of cervical dilatation. When a woman contacts a maternity hospital with a description of the symptoms of childbirth, cardiotocography is mandatory.
False contractions on CTG:
Despite the fact that a pregnant woman may have mild signs of labor, training contractions on CTG are easy to determine, since the main indicator will be the frequency of myometrial contraction of less than 110 beats / min.
With real contractions, a woman experiences systematic pain, the baby’s movements coincide with uterine contractions, and the baby’s heart rate rises. Since the manifestation of labor activity is quite obvious, the CTG will determine natural contractions.

With real contractions, a woman feels a sharp pain
In cases where contractions (real) are displayed on the CTG, the woman needs to prepare for the upcoming birth. If deviations are detected, it is CTG that can show serious violations that require emergency assistance.
With natural contractions, CTG will show the baby's frequent heartbeat and periodic contractions of the reproductive organ. The higher the lines on the graph rise, the more active the process of childbirth.
You should not try to understand on your own whether diagnostics gave good indicators or not. A specialist should deal with the decoding of CTG during contractions. We must not forget that any organism of both the mother and the fetus is individual. In addition, everyone's pregnancy has its own characteristics, so a deviation from the established norm is not always a reason for panic.
If you want to know how CTG goes, then watch this video:
The average norm in the process of delivery are indicators:
If CTG shows contractions, then the doctor examines the patient and decides on hospitalization.
During the time until the baby's head moves towards the exit, hardware sensors are attached to the belly of the expectant mother. The diagnostic method allows you to monitor the condition of the child even during childbirth.
The period of delivery significantly increases the load on the child's body - this phenomenon leads to a change in the frequency of contractions of the baby's heart muscle. That is why, in order to avoid critical situations and timely detect problems with the heart rhythm, obstetrician-gynecologists constantly monitor its performance. To assess the heart sounds of the fetus, the method of auscultation has long been used - listening to the baby's heartbeats with a wooden tube (obstetric stethoscope), which was placed on the belly of the expectant mother.
In the arsenal of the modern medical industry for these purposes there is complex ultrasound equipment - a cardiotocograph. The device, equipped with special sensors, simultaneously records uterine contractions and fetal heartbeat, which allows you to monitor the condition of mother and child. Assessing the dynamics of labor activity allows you to timely reduce the likelihood of asphyxia and oxygen starvation of the baby, to diagnose neurological disorders.
This type of examination of pregnant women has already become standard and is widely used in outpatient facilities for monitoring expectant mothers and maternity hospitals. The final data of the study (in the form of intersecting curves) are displayed on a calibration tape or special media - they can be saved. It happens that a woman comes to a medical and preventive consultation for a scheduled examination, she is given cardiotocography and it turns out that the process of labor has already begun!
Why does CTG show contractions, but a woman does not feel them at all? How to determine the harbingers of childbirth? How to distinguish false contractions from real ones? In this article, our readers will be able to find answers to these questions, as well as information about the cases in which the study is carried out and how contractions look on CTG.
The method of recording and analyzing the fetal heart rate is based on the Doppler effect - the device creates low-frequency signals that, reaching the uterus and heart muscle of the baby, are reflected and returned back. An electronic device picks up these signals and converts them into parameters of the intensity of contractions of the muscular layer of the uterus (myometrium) and the heart rate of the fetus.
All CTG indicators are displayed on the monitor of the device and recorded on paper tape in the form of a graphic image of two curves:

Modern equipment allows you to record the motor activity of the fetus, for this a woman needs to press a key on the remote control of the device, feeling the movement of the baby
Even with a normally occurring physiological process of delivery, the baby experiences many difficulties that are associated with an increase in the activity of all its systems. Pathological childbirth leads to a disruption in the supply of oxygen to the fetal organs, which leads to the development of hypoxia, which provokes serious problems in the functional activity of the child's body: stopping metabolic processes, the formation of irreversible reactions, and reducing adaptive capabilities.
Oxygen deficiency can be:
Severe hypoxia is accompanied by the appearance of areas with insufficient blood supply (ischemia), tissue death (necrosis) of various organs, and damage to the nervous system of the crumbs. The consequences of this pathological condition appear immediately after birth and require a long period of rehabilitation. The degree of risk of these problems depends on the duration of oxygen starvation.
Studies by modern scientists have established that a lack of oxygen for 7 minutes does not cause functional defects in the brain. However, after a quarter of an hour, signs of damage to the central nervous system appear, which will affect the functional and behavioral characteristics of the child. Longer hypoxia leads to fetal death.
The diagnostic procedure allows you to evaluate:

Three examinations are carried out for the expectant mother - at the time of her admission to the prenatal ward, at the discharge of fetal fluid and at the beginning of the period of fetal expulsion
The main purpose of the diagnostic procedure is to evaluate the baby's heartbeat. An obstetrician-gynecologist for half an hour (and in some cases more) studies whether the fetus is sufficiently supplied with oxygen. With its deficiency, a decrease (bradycardia) or an increase (tachycardia) of the pulse is observed. Cardiotocography is performed in all modern maternity hospitals during the entire period of delivery, especially if the woman in labor belongs to a high-risk group.
The procedure for diagnosing contractions is as follows:
Interpretation of the final data of CTG contractions is carried out to assess the condition of the infant during the period of strong true contractions of the muscles of the uterus and planning the tactics of childbirth. Here are some examples:
When deciphering the final CTG data, several methods are used, but most often the study parameters are evaluated in points or PSP is calculated - an indicator of the condition of the fetus.
It happens that the expectant mother experiences false contractions, which the famous English gynecologist John Braxton-Hicks called "training." Later, these short-term (up to 120 seconds), painless and irregular contractions of the myometrium, which occur in a pregnant woman in the third trimester, were named after the famous doctor. Many pregnant women experience fear when this kind of contractions appear. However, do not worry - they do not indicate any violations and are considered preparation for the upcoming delivery.
In late pregnancy, women take them for real, but training uterine contractions are not accompanied by cervical dilatation. The authenticity of contractions of the smooth muscle layer of the uterus is determined using a special physiological test, which is used to evaluate the function of the fetal heart muscle in relation to its motor activity and the close interaction of the infant's vascular system with the maternal placenta. If the level of these indicators is high, this characterizes the upcoming contractions.

The photo shows graphic recordings of CTG of real contractions.
In the absence of such "training" expectant mother should not worry - the female body knows how to behave correctly in the process of labor even without them. It is not difficult to distinguish false contractions from true ones - the latter cause painful sensations, are regularly repeated, accompanied by pain in the lower spine and spotting.
Based on the indicators of cardiotocography performed on the eve or during childbirth, a qualified specialist can assess the condition of the baby and plan the tactics of conducting the delivery process. With unsatisfactory results of CTG, the doctor takes all the necessary measures to identify the possible causes of fetal heart rhythm disturbances, eliminate them and designate the final term of natural childbirth.
In those situations where an urgent removal of the baby is required, surgical intervention is used: in the first stage of labor (before the onset of attempts), a caesarean section is performed, in the second - an episiotomy (dissection of the perineum). The use of obstetric forceps and vacuum extraction is used in extreme cases.
Summing up the above information, I would like to emphasize once again that the study of cardiotocography data during contractions can reduce the risk of severe asphyxia and fetal death, as well as the occurrence of neurological disorders in a newborn baby. And timely provided qualified assistance will positively affect the subsequent physical and neuropsychic development of the child.

Pregnancy is a very important moment in the life of a woman, and of the family as a whole. It brings not only joyful...

Reasons for the lack of ovulation, symptoms and signs The ovulatory function for a woman is the meaning laid down by the nature of her ...

Every woman knows that fertilization will not occur without ovulation. After all, they are inextricably linked with each other. Ovulation is...

Unfortunately, in recent years, infertility has deprived many women of the happiness of motherhood. It was with the request: "We can not ...

PROTECTION OF THE RIGHTS OF CONSUMERS OF CLOTHING AND SHOES As a rule, almost all unpleasant situations associated with purchases are associated with ...

Orthotic insoles are modified shoe inserts designed to support proper arch formation.

Most of those who passed through do not know anything about its features, since the moment of the sacrament ...

Everyone knows how important it is to properly raise a child so that in later life everything will work out for him ...
Our solar system is made up of the sun, planets orbiting it, and smaller celestial bodies. All...

Baptism for the Orthodox is the second (but in a certain sense the main) spiritual birth of a person, purification ...

You often meet people who try not to cook anything from eggplant. They all refer to...
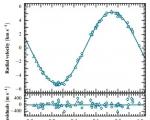
In the course of detailed observations as part of the WASP planetary search program, European astronomers have discovered a new ...

The mysterious interweaving of threads in the pattern of the lace fabric fascinates and attracts constant attention....

A dress or blouse with open shoulders should be in the wardrobe of every girl who wants to look romantic and...

Reasons for the lack of ovulation, symptoms and signs The ovulatory function for a woman is the meaning laid down ...

Every woman knows that fertilization will not occur without ovulation. After all, they are inextricably linked with each other ....